Smoking, Vaping and Mental Health
On November 15, 2019, Skyland Trail celebrated one year of being a Nicotine Free Campus! In November 2018, Skyland Trail became a 100% tobacco- and nicotine-free community and prohibited smoking, vaping and tobacco use in our residential mental health treatment programs and on all of our campuses.
Skyland Trail has joined a small group of residential psychiatric treatment organizations that are leading the field in integrating nicotine and tobacco cessation with behavioral health treatment and will contribute to a growing body of evidence and best practices for helping clients simultaneously learn to manage psychiatric symptoms and adopt skills and strategies for long-term health and wellness.
Smoking and Vaping Policies and Mental Health Treatment Facilities
Nicotine use has a long and entrenched history within the mental health system and among individuals with psychiatric illness.
Historically, psychiatric facilities have struggled to implement nicotine-free campuses because of the complexity of the issue and misconceptions surrounding smoking and psychiatric disorders. Common misconceptions include: smoking decreases symptoms and addressing nicotine dependence is less of a priority for someone with severe psychiatric issues.
Research suggests nicotine cessation treatment may be most effective when folded into other mental health care.
Less than half of mental health and substance abuse treatment centers (42 percent) offer tobacco cessation services and only 34 percent offer cessation counseling. (Centers for Disease Control and Prevention). On the other hand, most other healthcare facilities, including inpatient medical facilities and hospitals have implemented a policy shift towards smoke-free campuses in the last decade.
However, research suggests nicotine cessation treatment may be most effective when folded into other mental health care.
The American Psychiatric Association and National Institutes of Health favor treatment of smokers with mental health and substance use disorders. Some data suggests that bupropion and nicotine replacement therapy (NRT) may improve negative symptoms of schizophrenia, and that individuals on atypical antipsychotic drugs may be more responsive to bupropion than those on traditional antipsychotic medication.
For individuals engaged in treatment for substance use disorders, participation in smoking cessation efforts has been associated with a 25 percent greater likelihood of long-term abstinence from alcohol and other drugs (Prochaska et al. 2004).
In 2010, Miles McFall, PhD, at the University of Washington, Seattle, and colleagues reported in JAMA that when smoking cessation was integrated into treatment for veterans with post-traumatic stress disorder, the patients were more likely to be smoke-free 18 months later when compared with patients who attended smoking-cessation clinics separate from their PTSD treatment.
Smoking and Vaping among Individuals with Psychiatric Illness
While nicotine consumption has decreased in the general population, this has not been true for people with psychiatric disorders.
Approximately 25 percent of adults in the U.S. have some form of mental illness or substance use disorder, and these adults consume almost 40 percent of all cigarettes smoked by adults.
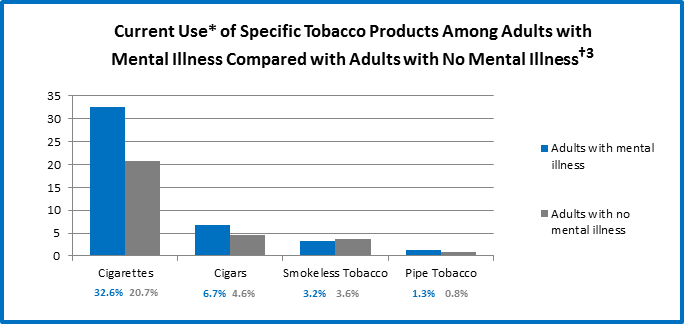
36.5% of adults with any mental illness reported current use* of tobacco in 2013 compared to 25.3% of adults with no mental illness.
* “Current Use” is defined as self-reported consumption of cigarettes, cigars, smokeless tobacco, and pipe tobacco in the past year and past month (at the time of survey).
† Data taken from the National Survey on Drug Use and Health, 2013, and refer to adults aged 18 years and older reporting any mental illness in the past year.
Vaping and Teens and Adolescents
According to a 2016 U.S. Surgeon General’s report, use of e-cigarettes or vaping pens is growing rapidly among youth and young adults. E-cigarettes are tobacco products that deliver nicotine.
In December 2018, the U.S. Surgeon General declared youth vaping an “epidemic.”
According to an advisory released by the Surgeon General in December 2018, e-cigarette use among U.S. middle and high school students increased 900% during 2011-2015, before declining for the first time during 2015-2017. However, current e-cigarette use increased 78% among high school students during the past year, from 11.7% in 2017 to 20.8% in 2018.

In 2018, more than 3.6 million U.S. youth, including 1 in 5 high school students and 1 in 20 middle school students, currently use e-cigarettes.
Many e-cigarettes come in flavors that appeal to kids and teens. Recent research shows that some of the chemicals used to make certain flavors may have health risks. The FDA currently is exploring banning flavored vapes and e-cigarettes to protect teens and adolescents.
Is vaping safe?
Studies show that many young people don’t realize that electronic cigarettes contain nicotine, which is a highly addictive drug. A single Juul cartridge contains as much nicotine as a pack of 20 tobacco cigarettes. The high level of nicotine may lead to higher rates of nicotine dependence among users, particularly young people.
According to the U.S. Surgeon General, in addition to nicotine, e-cigarettes can contain harmful and potentially harmful ingredients, including:
- ultrafine particles that can be inhaled deep into the lungs
- flavorants such as diacetyl, a chemical linked to serious lung disease
- volatile organic compounds
- heavy metals, such as nickel, tin, and lead
The Surgeon General reports that, “the health effects and potentially harmful doses of heated and aerosolized constituents of e-cigarette liquids—including solvents, flavorants, and toxicants—are not completely understood. However, e-cigarettes generally emit fewer toxicants than combustible tobacco products. We know that aerosol from e-cigarettes is not harmless.”
E-cigarettes may be used to deliver more than just nicotine. There has been reported use of certain types of e-cigarette-related products which deliver different forms of marijuana and other illicit drugs (Morean et al. 2015; Schauer et al. 2016). The tank systems, for example, have been used with liquid tetrahydrocannabinol (THC) or hash oil. Some personal vaporizer devices can be used with marijuana plant material or a concentrated resin form of marijuana called “wax.
Reports of vaping-related illnesses and even deaths are increasing. As of October 2019, federal and state officials report that vaping-related illness has affected more than 1,000 people nationwide and has been linked to at least 23 deaths in the U.S. Vaping-related illness in most cases has been linked to vaping products containing THC, the psychoactive compound in marijuana.
Nicotine Use and Mental Health
Helping patients quit smoking or stop using nicotine products is a critical component of promoting long-term health, preventing chronic disease, and ensuring the medications and interventions for psychiatric health are effective.
The following information comes from several studies by the CDC and SAMHSA regarding nicotine use among individuals with psychiatric illness and substance use disorders:
- The most common causes of death among people with mental illness are heart disease, cancer, and lung disease, which can all be caused by smoking.
- People with mental illness or substance use disorders die about 5 years earlier than those without these disorders. Many of these deaths are caused by smoking cigarettes.
- Drug users who smoke cigarettes are four times more likely to die prematurely than those who do not smoke.
- Nicotine has mood-altering effects that can temporarily mask the negative symptoms of mental illness, putting people with mental illness at higher risk for cigarette use and nicotine addiction.
- Tobacco smoke can interact with and inhibit the effectiveness of certain medications taken by mental health and substance abuse patients. (Centers for Disease Control and Prevention)
Nicotine Use and Teen Mental Health
Nicotine use by young adults may be particularly harmful. According to a 2016 Surgeon General’s report, “Compared with older adults, the brain of youth and young adults is more vulnerable to the negative consequences of nicotine exposure. The effects include addiction, priming for use of other addictive substances, reduced impulse control, deficits in attention and cognition, and mood disorders.”
According to a 2012 study by Goriounova and Mansvelder, the prefrontal cortex (PFC), the brain area responsible for executive functions and attention performance, is one of the last brain areas to mature and is still developing during adolescence. Smoking during adolescence increases the risk of developing psychiatric disorders and cognitive impairment in later life.
Quitting is Possible, Even for Individuals with a Mental Health Diagnosis
Myths about tobacco use among people with mental illness and substance abuse problems persist, such as:
- They are not interested in quitting.
- They cannot quit.
- Quitting interferes with recovery from mental illness or addictions.
- Tobacco is not as harmful as other substances.
- Tobacco is necessary for self-medication, and tobacco cessation would be too stressful.
- Tobacco cessation efforts might prevent treatment of other addictions.
It is true that, often, patients with mental illness have been smoking more years, and more cigarettes per day, than smokers in the general population. As a result, they may need more intensive treatment to help them quit.
However, with careful monitoring, delivering smoking cessation interventions does not interfere with treatments for mental illness and can actually be part of the treatment. (Centers for Disease Control)
Quitting Smoking and Vaping and Psychiatric Medications
When treating smokers with mental disorders, experts note, it is important to pay close attention to the medications they are taking because smoking can alter the levels of psychiatric medications in the bloodstream.
Tars in cigarette smoke affect the rate at which the liver metabolizes certain medications, causing blood levels of antidepressant and antipsychotic medications to decline, decreasing the effectiveness of the medication. If a patient quits smoking, blood levels rise and his or her old dose can become toxic. Fortunately, nicotine-replacement therapy does not interfere with antidepressant or antipsychotic medications.
The Skyland Trail Approach to Becoming a Nicotine-Free Mental Health Treatment Campus
The implementation plan was based on expertise from our Dual Diagnosis program, the treatment model used to help patients achieve and maintain sobriety from alcohol, marijuana, and other substances while simultaneously treating mental illnesses like depression, anxiety and schizophrenia.
Data Analysis
As a first step to address the issue, the clinical team examined the data. Current nicotine use status is collected for each patient at admission as part of the health and physical exam at the Glenn Family Wellness Clinic. Nicotine use status is collected again at discharge and recorded on the discharge summary by the primary counselor.
Key Findings from 2017 Data Analysis
- Nearly 40 percent of all patients used nicotine
- 10 percent of patients – 31 patients – started using nicotine while in treatment
- Only 3 percent of all patients quit smoking while in treatment
- 84 percent of patients who were nicotine users at admission refused tobacco intervention offered by their Skyland Trail psychiatrist during treatment
Nicotine Cessation Implementation
The clinical team concluded that more targeted intervention must take place at Skyland Trail to address the use of nicotine by our patient population and have assembled a Nicotine Cessation Task Force. The Nicotine Cessation Task Force proposed implementing a nicotine-free campus by November 15, 2018. Phase I focused primarily on drafting a policy to support the implementation of the nicotine ban, forming subcommittees to address specific components of the policy, and identifying a nicotine cessation curriculum to help clients quit.
Nicotine cessation resources provided to clients before admitting to residential mental health treatment
Phase II involved educating all Skyland Trail employees and community partners about the policy. Taskforce members also identified appropriate therapeutic interventions for patients who violate the nicotine ban, as well as incentives for adherence.
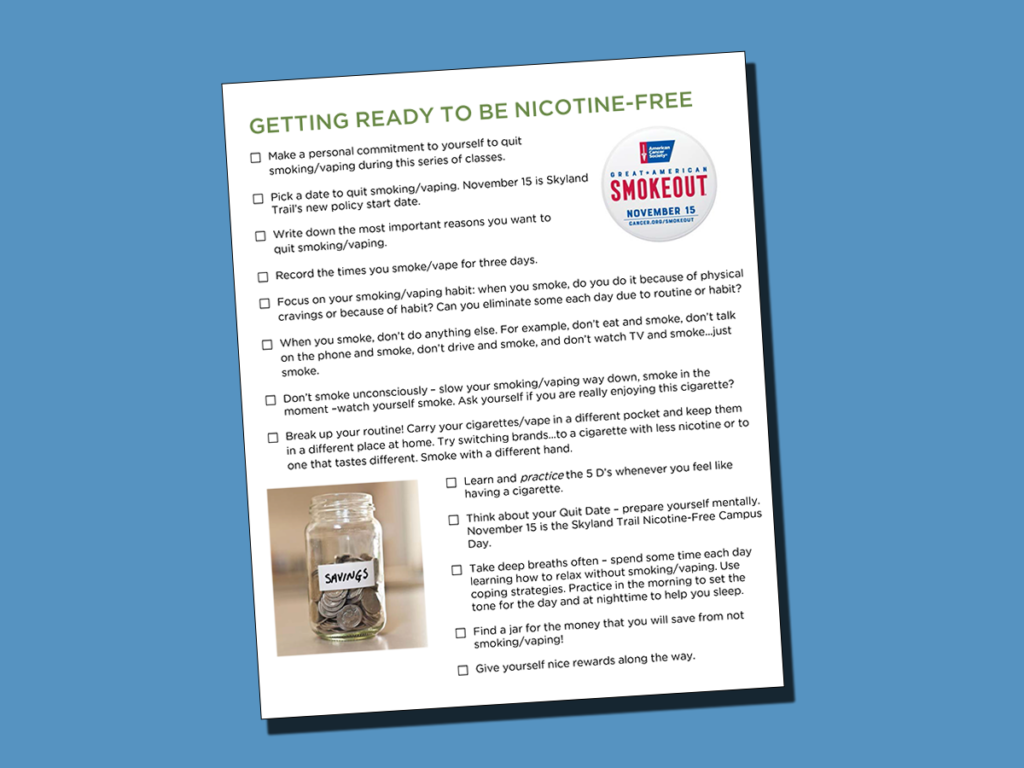
During Phase III, expanded nicotine cessation curriculum was offered for current clients. Interventions included psycho-educational and support groups, nicotine replacement therapies, and campus education events leading up to a “launch party” on campus on November 15, 2018.
Adult clients who admit to day treatment or residential treatment who currently smoke, vape, or use other nicotine products are enrolled in our tobacco cessation program. They participate in groups and may request nicotine replacement products or prescription medications if indicated.
Violations of the nicotine-free campus policy are addressed through a client’s overall wellness plan, and clients are given opportunities to address behaviors and receive support.
Evaluation
Skyland Trail continues to evaluate our nicotine cessation program and improve support to help clients admitting to our residential treatment program quit smoking or quit vaping.
Data collection is an important part of the evaluation process. Data is collected across the organization. Some key indicators include:
- comparison of clients who identify as smokers at discharge compared to admission
- number of interventions prescribed by Skyland Trail physicians or offered through the Glenn Family Wellness Clinic
- number of clients who complete the nicotine cessation curriculum while in treatment
References
Substance Abuse and Mental Health Services Administration, Center for Behavioral Health Statistics and Quality. The NSDUH Report: Adults With Mental Illness or Substance Use Disorder Account for 40 Percent of All Cigarettes Smoked [PDF–563 KB]. March 20, 2013. Rockville, MD [accessed 2016 May 18].
- U.S. Department of Health and Human Services. The Health Consequences of Smoking—50 Years of Progress: A Report of the Surgeon General. Atlanta: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health, 2014 [accessed 2017 Apr 20].
- U.S. Department of Health and Human Services. How Tobacco Smoke Causes Disease: What It Means to You. Atlanta: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health, 2010 [accessed 2017 Apr 20].
- Centers for Disease Control and Prevention. Quick Stats: Number of Deaths from 10 Leading Causes—National Vital Statistics System, United States, 2010. Morbidity and Mortality Weekly Report 2013:62(08);155. [accessed 2017 Apr 20].